
Some people consider vitamin B12 as a simple vitamin, which only affects the synthesis of red blood cells (figure 1, picture by Grok).
 So, if you do not have anaemia, you don’t have a B12 deficiency, and outside the setting of ‘anaemia’, B12 is useless. This is absolutely not correct. Vitamin B12 is a very important compound, it has multiple effects in our body, and is especially needed for optimal nerve function and for well-functioning mitochondria, the small organelles in our cells that are responsible for making energy.
So, if you do not have anaemia, you don’t have a B12 deficiency, and outside the setting of ‘anaemia’, B12 is useless. This is absolutely not correct. Vitamin B12 is a very important compound, it has multiple effects in our body, and is especially needed for optimal nerve function and for well-functioning mitochondria, the small organelles in our cells that are responsible for making energy.
B12 -as a medication- has also been used by intensive care doctors in severely ill people. There are several interesting papers on the use of hydroxocobalamin for people who suffer from (refractory) vasoplegia after cardiopulmonary bypass surgery, heart surgery. Vasoplegia (vascular shock) is a clinical syndrome characterised by severe vasodilatation (widening of the blood vessels) of the smaller arteries and arterioles, hypotension (very low blood pressure), and low systemic vascular resistance that does not respond to treatments with multiple vasopressor medications, medications that should promote the vessels to get narrower and blood pressure to increase. I have selected three papers in this area to explain this complex medical topic further.
The 2018 Shah paper, see figure 2:
Full reference: Shah PR, Reynolds PS, Pal N, Tang D, McCarthy H, Spiess BD. Hydroxocobalamin for the treatment of cardiac surgery-associated vasoplegia: a case series. Can J Anaesth. 2018 May;65(5):560-568. English. doi: 10.1007/s12630-017-1029-3. Epub 2017 Dec 5. PMID: 29209927.
Link to the paper: https://link.springer.com/article/10.1007/s12630-017-1029-3
In this paper, already published 8 years ago (!), doctors from Richmond, Virginia, report their experience with using a hydroxocobalamin (B12) infusion as a potential rescue adjunct for refractory vasoplegia during cardiopulmonary bypass surgery. They studied a series of 33 individuals, who underwent cardiac surgery between 1 January 2013 and 31 December 2015. Patients were given intravenous infusion of methylene blue or vitamin B12 (hydroxocobalamin) for severe not-responsive hypotension during, or immediately following, surgery.
Compounds as methylene blue and hydroxocobalamin are mechanistically unique and thought to work through nitric oxide–based mechanisms to induce vasoconstriction. When you ask Google’s AI, it reports that Vitamin B12 (cobalamin) also acts as a direct scavenger of reactive oxygen species (ROS), particularly superoxide (O2-), with activity comparable to that of superoxide dismutase (SOD). It reduces oxidative stress by scavenging (‘hunting and grabbing’) radicals and preserving glutathione, protecting DNA and cells from damage. It is effective in mitigating ischaemia/reperfusion injury and supporting neural health.
In the study by Shah et al, individuals had received methylene blue and/or hydroxocobalamin (5 g, Cyanokit), administered as an intravenous infusion over a 15 minute period. The overall finding and conclusion of the paper is that there was considerable diversity in the response of an individual to B12; the authors suggested that this may have depended on both the patient’s preoperative condition and the fact that the timing of the administration was not standardized. Nevertheless, in their opinion, vitamin B12 may provide a useful alternative or additional therapy to treat refractory hypotension and vasoplegia, but -as they were looking back- they state that prospective controlled clinical trials to assess the true efficacy of the therapy are needed.
A second paper on this topic (figure 3) was published in 2025 by a group of doctors in Cairo, Egypt, and it describes the prophylactic use of hydroxocobalamin in patients at high risk of developing vasoplegia after cardiopulmonary bypass. So, a high dose of B12 is administered to assess whether this can prevent severe illness.
Full reference: Salah D, Ahmed S, Ibrahim DA. Use of Hydroxycobolamin in the Prevention of Vasoplegic Syndrome in Adult Patients Undergoing Cardiopulmonary Bypass: A Controlled Prospective Trial. J Cardiothorac Vasc Anesth. 2025 May;39(5):1180-1187. doi: 10.1053/j.jvca.2025.02.001. Epub 2025 Feb 5. PMID: 40055025.
Link to the paper: https://www.jcvaonline.com/article/S1053-0770(25)00114-4/abstract
How did they treat the participants? At the end of cardiopulmonary bypass (CPB), the participants were assigned by chance into two groups: 30 individuals in group I received hydroxocobalamin 5 g intravenously via the central venous catheter as a bolus over 15 minutes reconstituted in 200 ml of normal saline, and 30 individuals in group II (the so-called ‘control group’) received 200 mL of normal saline intravenously over 15 minutes. When they collected all information, it turned out that the B12 prevention group showed higher arterial blood pressure 30 and 60 minutes after CPB separation, they required lower amounts of vasopressor treatment (norepinephrine) at minutes 30 and 60 after CPB separation, as well as total dose norepinephrine equivalent. Also, lower serum lactate concentrations (a sign of poor blood perfusion of the body’s tissues), and lower incidence of vasoplegic shock syndrome and norepinephrine-resistant refractory vasoplegia were noted. The number of days that a patient neededa rtifical ventilation (3.8 vs 4.1 days), the length of stay in the intensive care unit (6.2 vs 7.0 days), the length of the stay in the hospital, and the number of participants who did not survive this severe illness (1 of 30 vs 3 of 30) were lower or less frequent in the B12 group, but the authors note that these differences were not statistically significant.
The third paper which we discuss briefly, is a recent article from a group of doctors in Pittsburgh, PA, USA; figure 4 shows what we call the graphical abstract of this paper.
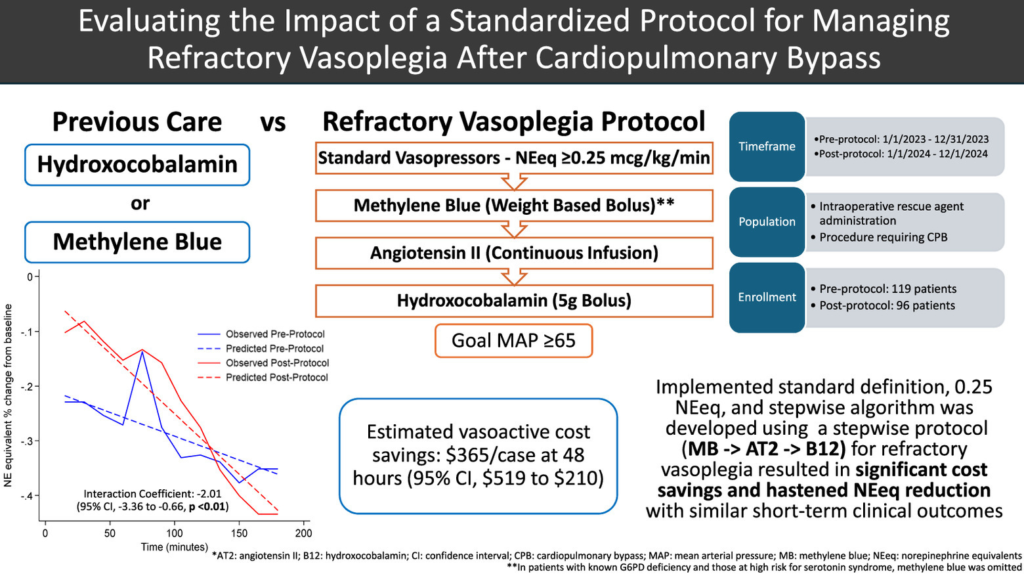
Full reference: Teletnick A, Suh K, Boisen M, Brown JA, Cabral B, Murray H, Paley C, Sullinger D, Sultan I, Thoma F, Williams J, Subramaniam K, Rivosecchi RM. Evaluating the Impact of a Standardized Protocol for Managing Refractory Vasoplegia After Cardiopulmonary Bypass. J Cardiothorac Vasc Anesth. 2026 Feb 6:S1053-0770(26)00110-2. doi: 10.1053/j.jvca.2026.02.003. Epub ahead of print. PMID: 41765732.
Link to the paper: https://www.jcvaonline.com/article/S1053-0770(26)00110-2/fulltext
This article describes a prospective evaluation of the haemodynamic impact and cost-effectiveness of a standardized protocol for treating people who develop refractory vasoplegia after cardiopulmonary bypass. In this paper, refractory vasoplegia was defined as at least 0.25 μg/kg/min norepinephrine equivalents (NEeq), and a stepwise rescue treatment protocol was developed, starting with methylene blue, then giving angiotensin II and subsequently hydroxocobalamin (see figure 4).
The authors assessed the effects of the rescue intervention by looking back in time and comparing patients undergoing CPB after the implementation of this new protocol with those undergoing CPB before protocol implementation, the latter group receiving rescue agents at the discretion of the managing ICU doctor. Again, the hydroxocobalamin dose was 5 g, the so-called Cyanokit.
Their findings in short: they observed a faster reduction in vasopressor therapy and lower associated costs of the treatment with the rescue intervention. They did, however, not find any differences in short-term clinical outcomes between groups.
So, to summarize these three papers, it appears that hydroxocobalamin has an important role in treating the so-called vasoplegia in critically ill patients after heart surgery. However, several additional questions arise. For example, is there an optimal dose of hydroxocobalamin, and, also, can repeated administrations of B12 add to a prolonged or sustained effect? The findings of the Egyptian group regarding shorter durations of mechanical ventilation and shorter stays in the intensive care unit and in the hospital are very interesting and warrant further investigation.
Another interesting aspect to consider is that of pre-operative B12 status. As a doctor who is interested in the effects of B12 deficiency, I ask myself: do individuals who are undergoing surgery while having B12 insufficiency or deficiency have a higher risk of becoming severely ill and developing vasoplegia? Especially now that we see more and more people adopting a plant-based diet, who sometimes develop B12 deficiency despite supplementation. I hope that the results described in these three papers will encourage more researchers and clinicians to further explore the intriguing effects of B12.
Parts of this blog have also been published in CluB-12’s March 2026 Newsletter.
For translation into Dutch, copy this blog to Google Translate



Recente reacties