door bhrw | aug 5, 2025 | diabetes, gezondheidszorg
Zo’n 90 jaar geleden bracht uitgevers-maatschappij Kosmos het Dieet-kookboek voor suikerzieken uit.
Een handzaam boekje vol tabellen en recepten. Tabellen met het koolhydraat- en eiwitgehalte van gerechten.
Recepten voor verantwoorde gerechten voor mensen met diabetes, en wel de variant die we nu type 1 diabetes noemen.
Van bloemkool- en spinaziesoep, tot toespijzen van aardbeiendparfait tot vanillevla en vruchtenvla, en enkele cocktails.
Je wordt vrolijk van de cokcktails die op blz 53 zijn beschreven, bv de Turfclub: 20 c.c. Rhum, 40 c.c. Cognac, paar dr. Angustora (een kruidenbitter).
Er was zelfs een lijst van voedingsmiddelen met hun vermoede gehalte aan A, B, C, D en E vitamine. Met nog bar weinig onderscheid tussen de B vitamines, bv vitamine B12 was nog niet ontdekt.
Acht a negen jaar eerder, in 1926, was de zogenaamde “antipernicieuze factor” ontdekt door George Minot en William Murphy. De bron was de lever, de basis voor de behandeling van mensen met B12 tekort in de jaren 30 en 40. Pas in 1948 werd vitamine B12 als aparte stof geïsoleerd.
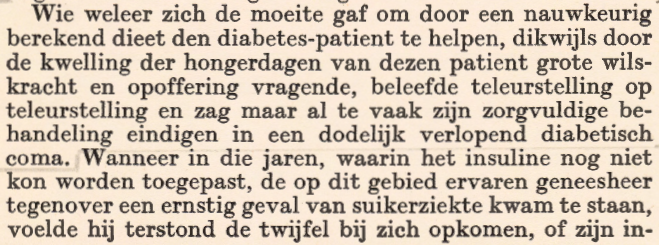
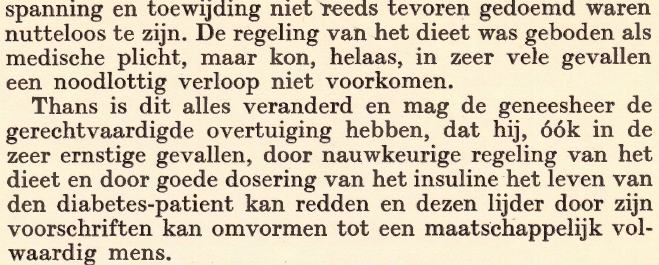
Het voorwoord van het boek werd geschreven door dr. Jac. J. de Jong, die terecht stilstond bij de immense landverschuiving die was opgetreden door het beschikbaar komen van insuline, als behandeling van type 1 diabetes, vanaf 1922.
Twee citaten:
door bhrw | mrt 10, 2025 | diabetes, Lifelines, schildklier, stofwisselingsziekten, wetenschap
Iedere twee jaar wordt ter ere van Ernst Laqueur, die wordt beschouwd als een van de grondleggers van de moderne endocrinologie, een lezing gehouden door een onderzoek(st)er die in de afgelopen decennia veel voor de (neuro)endocrinologie heeft betekent. Het bestuur van de NVE selecteert de Laqueur lecturer.

(meer…)
door bhrw | jan 8, 2025 | diabetes, gezondheidszorg

Deze maand wordt gevierd dat ruim 10 jaar geleden het Flash Glucose Monitoring systeem van Abbott, de FreeStyle Libre, op de Nederlandse markt werd geïntroduceerd. Continue meting van de onderhuidse glucose waarden is een geweldige aanwinst voor mensen met diabetes. Inmiddels is al versie 3 van de FreeStyle Libre beschikbaar; deze versie stuurt in realtime de resultaten van de glucose meting naar je smartphone.
Voor een uitleg van dit syteem, zie: https://www.freestyle.abbott/nl-nl/producten/freestylelibre-3.html
Ervaringen
Al in 2014 mocht ik twee weken lang de Freestyle Libre ervaren, zie: https://gmed.nl/abby-my-new-girl-friend/. Destijds schreef ik onder andere:

“Every minute she measures the glucose from below my skin, which is a reasonable estimate of my blood glucose. She comes with a separate receiver, a small device which records all measurements and presents a sort of logbook. All I have to do is keep the receiver in front of the sensor, and it reads the current value, and also collects the recordings / measurements of the previous 8 hours. The absolute beauty is that there is no need for calibration. I can swim (although I did not do that yet), take my shower every day, jog, cycle, etc. etc. Sleeping is no problem, I do even not feel the device when I am lying on my left side. She is glued tightly to my skin, although I am a bit careful when putting on cloths so that I am not pulling too much. Insertion of the sensor was without problems, took exactly one minute (and I am a slow learner). Until now, Abby works like a breeze. And I get some nice insights into my blood glucose excursions during the day, for instance after a meal.”
In 2015 vertelde Stephen Dixon, anchorman van Sky News, op een groot diabetes congres over zijn ervaringen met het systeem. Dixon heeft sinds zijn 17e type 1 diabetes, en gebruikte tot zijn grote tevredenheid de FreeStyle Libre. Dixon vertelde over zijn ervaringen met diabetes, het gebruik van de FreeStyle Libre in vergelijking met gewone bloedglucose metingen (tevoren deed hij minstens 15 vingerprikken en bloedglucose metingen per dag), en het ‘embarrassing’ gevoel om aan tafel je bloedglucose te moeten meten.

Hij beschreef het verschil als “Now I know where I am AND where I go with my glucose levels”.
Beschikbaarheid
Toch was niet alles koek en ei in het begin. Aanvankelijk waren er (te) weinig sensoren beschikbaar in Nederland. Een studie in de Isala klinieken kon door het gebrek aan sensoren niet eens van start gaan. Bovendien waren zorgverzekeraars niet of nauwelijks bereid om dit systeem voor hun patienten te vergoeden. ‘Voldoet niet aan de stand van de wetenschap’, aldus OHRA volgens een tweet in 2015 van Stefanie Rondags, die zelf al lange tijd gebruikster is van de FreeStyle Libre.
Dat ‘zeurde no door’ tot tenminste 2018. Sommige zorgverzekeraars hebben in 2018 regelmatig geweigerd om een machtiging voor vergoeding af te geven omdat ‘de firma Abbott de FreeStyle Libre nog onvoldoende kan leveren’. Maar het tegengestelde gold gelukkig ook. Ik had in september 2018 een uitgebreid telefoongesprek met iemand van de zorgverzekeraar Zilveren Kruis, die juist aangaf alle aanvragen goed te keuren, die aan de criteria voldoen: ‘Dan kunnen onze verzekerden snel profiteren als de sensoren dadelijk in oktober (2018) breder beschikbaar komen’.
Bewijs
Inmiddels is er veel wetenschappelijk bewijs voor de effectiviteit en het belang van systemen als de FreeStyle Libre. Ik verwijs onder andere naar de mooie studies, die in Nederland zijn uitgevoerd ponder leiding van de hoogleraren Henk Bilo en Rijk Gans, en die zijn samengevat in het proefschrift, waarop de internist Annel Lameijer -mede met begeleiding van deze hoogleraren en de internist Peter van Dijk- in september 2024 promoveerde. U kunt haar mooie proefschrift hier vinden en downloaden: https://www.rug.nl/umcg/phd-ceremonies-umcg?hfId=123971

Kwaliteit van leven
In 2022 onderzocht een groep studenten Geneeskunde hier in Groningen de effecten van gebruik van een glucose sensor op de kwaliteit van leven. Hun conclusie was verpletterend:
“Sensortechnologie biedt aan mensen met type 1-diabetes de mogelijkheid om het verloop van de glucosewaarde nauwgezet te volgen. Bij bepaalde typen sensoren is er tevens de mogelijkheid van alarmering bij (dreigende) hypoglykemie. Wij onderzochten in een retrospectieve studieopzet of de kwaliteit van leven van mensen met type 1-diabetes veranderd is door het gebruik van continue glucosemonitoring via een sensor. In totaal werden de vragenlijsten − deels gebaseerd op de PAID en Angst voor Hypoglykemie Vragenlijst en deels op de EQ5L kwaliteit van leven-schaal − door 105 mensen ingevuld. De gemiddelde leeftijd was 50 (spreiding van 18 tot 76) jaar. In totaal maakten 33 (31%) personen gebruik van Flash Glucose Monitoring (FGM) en 72 (69%) van Real-Time Continue Glucose Monitoring (RT-CGM). Er was een sterke en significante toename van de gerapporteerde kwaliteit van leven in alle domeinen. Een significante daling van het HbA1c-gehalte werd vastgesteld bij die mensen die de sensortechnologie toepasten ter verbetering van de glykemische regulatie. Wij concluderen dat er sprake is van een sterke verbetering van de kwaliteit van leven bij het gebruik van FGM of RT-CGM in vergelijking met de vingerprikmethode bij mensen met type 1-diabetes. Daarnaast verbeterde de glucoseregulatie aanzienlijk.”
Technologie
Continue glucose monitoring is slechts één onderdeel van de optimale (zelf)behandeling van mensen met type 1 diabetes. Tesamen met een insuline-pomp, aangestuurd door een goede behandelalgoritme voor de toediening van insuline, is het een technologische oplossing voor veel problemen die inherent zijn aan het zo goed mogelijk reguleren van je diabetes. Een voorbeeld van zo’n systeem is het mylife CamAPS FX systeem, dat inmiddels ook enkele jaren in Nederland beschikbaar is. Het totale systeem bestaat uit de myLife YpsoPump insuline pomp, de Dexcom G6 glucose sensor of de FreeStyle Libre, en het verbindende CamAPS FX software systeem, dat is ontworpen door professor Roman Hovorka, een genie op het gebied van diabetes en closed-loop software.
Kijk hier naar de opnames van een webinar, waarin dit systeem wordt uitgelegd. De link is: https://www.youtube.com/watch?v=FNzAE-6A1-4
door bhrw | nov 15, 2024 | diabetes

Mijn onderzoeksgroep publiceerde recent een artikel, waarin we in een groep mensen met type 1 diabetes hebben gekeken naar het probleem van het niet aanvoelen van hypo’s (impaired unawareness of hypoglycaemia, IAH), en hoe dit over de tijd varieert. Al eerder hebben we aangetoond dat mensen met type 1 diabetes, bij wie nog enige residuele insuline secretie aanwezig is (hetgeen wordt gedetecteerd dat in het serum nog C-peptide te meten valt) een kleinere kans hebben op IAH. In deze sytudie bevestigen we dit, en beschrijven we ook d ekarakteristieken van mensen bij wie IAH weer verdwijnt.
Het abstract van de studie:
Aims: To describe the change in impaired awareness of hypoglycaemia (IAH) over time and to identify factors associated with this change in the Dutch Type 1 Diabetes biomarkers cohort (NCT04977635).
Methods: A prospective cohort of type 1 diabetes patients, with C-peptide <300 pmol/L, who had completed the Clarke questionnaire, to determine IAH status, at baseline and after 2 years. Changes in awareness status were defined and compares as follows: unchanged normal awareness (NAH) versus unchanged IAH, new IAH versus reversal of IAH. Multivariate logistic regression models were fitted using forward and backward stepwise selection using a 0.10 P-value cut-off, and stepwise backward selection using AIC criteria.
Results: A total of 431 out of 611 participants were included. The baseline prevalence of IAH was 17 % and 20 % after 2 years. The incidence proportion of new IAH and reversal of IAH were, 9.5 % and 31 %, respectively. For every 2.7-fold increase in C-peptide, the odds of IAH decrease by 58 %. A 1-unit increase in BMI over the 2-year follow-up period is associated with a 5.27-fold increase in the odds of reversing IAH.
Conclusions: Higher C-peptide levels are protective against new IAH, and an increase in BMI over time is associated with the reversal of IAH.
Het volledige artikel vindt u hier: https://www.sciencedirect.com/science/article/pii/S1056872724002198
door bhrw | mrt 1, 2024 | diabetes, gezondheidszorg, wetenschap
Endocrine-Disrupting Chemicals and type 2 diabetes: what is their relationship?
Summary of all research performed in the Department of Endocrinology of the UMCG, on endocrine disruptors, obesity and type 2 diabetes through a personal researcher grant awarded by DiabetesFonds Nederland to dr Jana van Vliet-Ostaptchouk.
Endocrine disrupting chemicals (EDCs) are exogenous compounds with the potential to disturb hormonal regulation and the endocrine system, consequently affecting health and reproduction in animals and humans (1). EDCs can interfere with the production, release, metabolism, and elimination of or can mimic the occurrence of natural hormones. Parabens, bisphenols and phthalates are EDCs which have in common that even though having lipophilic properties, they are quickly metabolized into more water-soluble chemicals. These chemicals in turn are easily excreted via the kidneys from the body. Due to their short half-lives of less than 24 hour, these chemicals are considered to be non-persistent (2-4). In contrast, persistent EDCs are often more resilient to metabolic degradation, making it harder to excrete these chemicals. For example, polychlorinated biphenyls (PCBs) contain chlorine atoms, which make hydroxylation by the liver much harder and leads to half-live times of months to decades. As a result, PCBs are still widely detected in blood regardless of the fact that they have been banned at least in part in Europe in 1985. Even though non-persistent EDCs are easily metabolized and excreted, their use in a wide variety of daily used consumer products has led to an ubiquitous exposure around the world.
For example, bisphenol A (BPA), 2,2-bis(4-hydroxyphenyl)propane, is a synthetic compound that is widely used as a monomer in polycarbonate plastics and epoxy resins, being one of the world’s highest production volumechemicals (Source: paper #13, Environ Int 2015). This means that humans are widely exposed to chlorinated derivatives and structural analogs of bisphenol A.
Exposure to EDCs may play an important role in the global escalating incidence of type 2 diabetes observed in the last few decades (5). Based on the observations that EDCs interfere with the body’s endocrine system, a connection between EDC and altered glucose metabolism and increased risk for T2D is proposed. This project aimed to investigate how EDC determine the risk of T2D and to pinpoint the underlying pathophysiological mechanisms. Our hypothesis was that chronic daily exposure to EDC increases the risk of developing T2D through a cascade of adverse metabolic changes. We performed systematic analysis of EDC-related changes (single and multiple EDC effects) in metabolic functioning, epigenetics and gene expression patterns, combined with an analysis of individual genetic profiles and lifestyle. This strategy aimed to uncover mechanisms underlying EDC-induced metabolic dysregulation. Our main objectives were:
- To investigate whether exposures to EDC as measured in urine increase the risk of T2D and how this risk is modified by lifestyle and genetic predisposition
- To examine the effects of EDC on metabolism and to establish EDC-related alterations in gene function (i.e. DNA methylation and gene expression)
Click on ‘meer’ to read further..
(meer…)
door bhrw | dec 4, 2023 | diabetes, gezondheidszorg, wetenschap

Background
Type 2 diabetes disproportionately affects individuals of non-White ethnicity through a complex interaction of multiple factors. Therefore, early disease detection and prediction are essential and require tools that can be deployed on a large scale. We aimed to tackle this problem by developing questionnaire-based prediction models for type 2 diabetes prevalence and incidence for multiple ethnicities.
Methods
In this proof of principle analysis, logistic regression models to predict type 2 diabetes prevalence and incidence, using questionnaire-only variables reflecting health state and lifestyle, were trained on the White population of the UK Biobank (n = 472,696 total, aged 37–73 years, data collected 2006–2010) and validated in five other ethnicities (n = 29,811 total) and externally in Lifelines (n = 168,205 total, aged 0–93 years, collected between 2006 and 2013). In total, 631,748 individuals were included for prevalence prediction and 67,083 individuals for the eight-year incidence prediction. Type 2 diabetes prevalence in the UK Biobank ranged between 6% in the White population to 23.3% in the South Asian population, while in Lifelines, the prevalence was 1.9%. Predictive accuracy was evaluated using the area under the receiver operating characteristic curve (AUC), and a detailed sensitivity analysis was conducted to assess potential clinical utility. We compared the questionnaire-only models to models containing physical measurements and biomarkers as well as to clinical non-laboratory type 2 diabetes risk tools and conducted a reclassification analysis.
Findings
Our algorithms accurately predicted type 2 diabetes prevalence (AUC = 0.901) and eight-year incidence (AUC = 0.873) in the White UK Biobank population. Both models replicated well in the Lifelines external validation, with AUCs of 0.917 and 0.817 for prevalence and incidence, respectively. Both models performed consistently well across different ethnicities, with AUCs of 0.855–0.894 for prevalence and 0.819–0.883 for incidence. These models generally outperformed two clinically validated non-laboratory tools and correctly reclassified >3,000 additional cases. Model performance improved with the addition of blood biomarkers but not with the addition of physical measurements.
Interpretation
Our findings suggest that easy-to-implement, questionnaire-based models could be used to predict prevalent and incident type 2 diabetes with high accuracy across several ethnicities, providing a highly scalable solution for population-wide risk stratification. Future work should determine the effectiveness of these models in identifying undiagnosed type 2 diabetes, validated in cohorts of different populations and ethnic representation.

You can download the full article HERE.




Recente reacties